








World Pneumonia Day is observed on November 12, every year. It provides an annual forum for the world to stand together and demand action in the fight against pneumonia. The theme for 2019 is: Stop Pneumonia By Initiatives. Stop Pneumonia is an initiative that provides a voice for communities who suffer from the devastating consequences of the disease and who lack access to lifesaving interventions.
Pneumonia is a preventable and treatable disease that sickens about 155 million children under 5 and kills 1.6 million each year. This makes pneumonia the number one killer of children under-5, claiming more young lives than AIDS, malaria, and measles combined.
However, there are effective vaccines against the two most common causes of deadly pneumonia. Pneumonia is one of the commonest manifestations of Pneumococcal disease. It may occur in subjects of any age, but it is encountered most frequently in the very young and in the old.
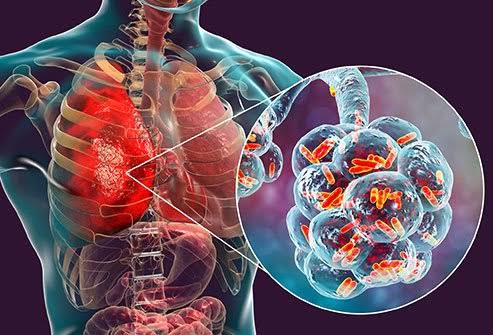
Pneumonia spreads from person to person by droplet infection. Clinical observations and studies in experimental animals suggest that most causes of pneumonia result from aspiration of nasopharyngeal secretions containing pneumococci into alveoli. Once established in the lung, pneumococci may spread to adjacent pleura or pericardium. About one-third of patients with pneumococcal pneumonia have a positive blood culture, and bacteria may spread through the systemic circulation to reach the joints, eyes, or other distant sites.
An increase in susceptibility to pneumococcal infection may result from defects in either local or systemic defence mechanisms. Factors that impair the cleansing action of the respiratory cilia favour aspiration of infected nasopharyngeal secretions into alveoli. These include cold, anesthesia, alcohol intoxication, drug overdose, and viral infection of the respiratory tract.
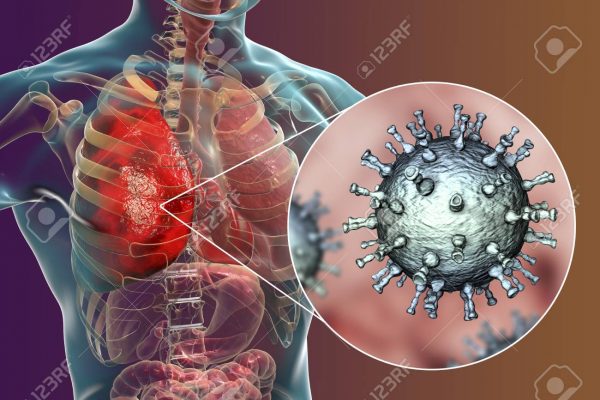
Viral infec¬tions such as influenza or measles increase respiratory tract sec-retions, damage the ciliated epithelium of the respiratory tract and interfere with func¬tion of the body system. It is therefore not surprising that epidemics of influenza are often followed by an increase in the incidence of pneumonia, especially among the elderly.
Patients with sickle cell disease have an increased incidence of pneumococcal infection. Splenic dysfunc¬tion and an abnormality in the alternative complement pathway have been identified as factors predisposing to pneumococcal infection in patients with this condition.
The onset of pneumonia is usually sudden, although there may be a his¬tory of a recent preceding upper respiratory tract infection. Fever is usually the first clinical feature of pneumonia. It is frequently accompanied by rigours. The patient feels ill and weak. Headache may be severe.
Chest pain usually appears in the course of illness. This pain is sharp and stabbing and is aggravated by deep inspiration or coughing. Cough may be absent at the onset of the illness but, in most patients, it becomes a prominent symptom. Cough is initially non¬productive and painful. Subsequently, it becomes productive of blood-tinged ‘rusty’ sputum.
Finally, the sputum becomes frankly purulent. The patient’s breathing is distressed and the nostrils may dilate on inspiration. Cyanosis may be present as a result of diminished alveolar ventilation or shunting of desiderated blood through the consolidated lung. Chest movement is diminished on the affected side. Jaundice may be present, while elderly patients with pneumonia frequently become confused and disorientated.
Global community is therefore urged to consider the massive problems of Pneumonia. Better yet, take a moment to consider what can be done to solve the problem. Health care providers, researchers, policy makers and the greater public health community all need to contribute, if we are to make rapid, substantial progress towards reducing disease and death due to Pneumonia. Progress is being made but much more can be done.
INITIATE ACTION NOW AGAINST PNEUMONIA TO SAVE OUR CHILDREN!
Comments are closed for this post.